The curve of mortality rate has been flattening on Worldometers. Means the number of recoveries is starting to rise faster than the number of dead.
Last edited:
Learned this morning that one our our local suppliers went down due to a positive COVID-19 case at their facility.
The learned one of my program's Quality Control reps went into that supplier last week.
They are 100% getting send home now but now I fear COVID-19 has infected my job.
I'm working from home 60% of the time now but still doesn't sit well with me knowing tomorrow I have to work on site.
Long Island btw, working Defense.
For the amount of noise about chloroquine from Trump and others, at this point it would have to be assumed that it's either not at all effective or marginal at best.
Has anyone seen this to be totally accurate where you are?
"I am an ER MD in New Orleans. Class of 98. Every one of my colleagues have now seen several hundred Covid 19 patients and this is what I think I know.
Clinical course is predictable.
2-11 days after exposure (day 5 on average) flu like symptoms start. Common are fever, headache, dry cough, myalgias(back pain), nausea without vomiting, abdominal discomfort with some diarrhea, loss of smell, anorexia, fatigue.
Day 5 of symptoms- increased SOB, and bilateral viral pneumonia from direct viral damage to lung parenchyma.
Day 10- Cytokine storm leading to acute ARDS and multiorgan failure. You can literally watch it happen in a matter of hours.
81% mild symptoms, 14% severe symptoms requiring hospitalization, 5% critical.
Patient presentation is varied. Patients are coming in hypoxic (even 75%) without dyspnea. I have seen Covid patients present with encephalopathy, renal failure from dehydration, DKA. I have seen the bilateral interstitial pneumonia on the xray of the asymptomatic shoulder dislocation or on the CT's of the (respiratory) asymptomatic polytrauma patient. Essentially if they are in my ER, they have it. Seen three positive flu swabs in 2 weeks and all three had Covid 19 as well. Somehow this ***** has told all other disease processes to get out of town.
China reported 15% cardiac involvement. I have seen covid 19 patients present with myocarditis, pericarditis, new onset CHF and new onset atrial fibrillation. I still order a troponin, but no cardiologist will treat no matter what the number in a suspected Covid 19 patient. Even our non covid 19 STEMIs at all of our facilities are getting TPA in the ED and rescue PCI at 60 minutes only if TPA fails.
Diagnostic
CXR- bilateral interstitial pneumonia (anecdotally starts most often in the RLL so bilateral on CXR is not required). The hypoxia does not correlate with the CXR findings. Their lungs do not sound bad. Keep your stethoscope in your pocket and evaluate with your eyes and pulse ox.
Labs- WBC low, Lymphocytes low, platelets lower then their normal, Procalcitonin normal in 95%
CRP and Ferritin elevated most often. CPK, D-Dimer, LDH, Alk Phos/AST/ALT commonly elevated.
Notice D-Dimer- I would be very careful about CT PE these patients for their hypoxia. The patients receiving IV contrast are going into renal failure and on the vent sooner.
Basically, if you have a bilateral pneumonia with normal to low WBC, lymphopenia, normal procalcitonin, elevated CRP and ferritin- you have covid-19 and do not need a nasal swab to tell you that.
A ratio of absolute neutrophil count to absolute lymphocyte count greater than 3.5 may be the highest predictor of poor outcome. the UK is automatically intubating these patients for expected outcomes regardless of their clinical presentation.
An elevated Interleukin-6 (IL6) is an indicator of their cytokine storm. If this is elevated watch these patients closely with both eyes.
Other factors that appear to be predictive of poor outcomes are thrombocytopenia and LFTs 5x upper limit of normal.
Disposition
I had never discharged multifocal pneumonia before. Now I personally do it 12-15 times a shift. 2 weeks ago we were admitting anyone who needed supplemental oxygen. Now we are discharging with oxygen if the patient is comfortable and oxygenating above 92% on nasal cannula. We have contracted with a company that sends a paramedic to their home twice daily to check on them and record a pulse ox. We know many of these patients will bounce back but if it saves a bed for a day we have accomplished something. Obviously we are fearful some won't make it back.
We are a small community hospital. Our 22 bed ICU and now a 4 bed Endoscopy suite are all Covid 19. All of these patients are intubated except one. 75% of our floor beds have been cohorted into covid 19 wards and are full. We are averaging 4 rescue intubations a day on the floor. We now have 9 vented patients in our ER transferred down from the floor after intubation.
Luckily we are part of a larger hospital group. Our main teaching hospital repurposed space to open 50 new Covid 19 ICU beds this past Sunday so these numbers are with significant decompression. Today those 50 beds are full. They are opening 30 more by Friday. But even with the "lockdown", our AI models are expecting a 200-400% increase in covid 19 patients by 4/4/2020.
Treatment
Supportive
worldwide 86% of covid 19 patients that go on a vent die. Seattle reporting 70%. Our hospital has had 5 deaths and one patient who was extubated. Extubation happens on day 10 per the Chinese and day 11 per Seattle.
Plaquenil which has weak ACE2 blockade doesn't appear to be a savior of any kind in our patient population. Theoretically, it may have some prophylactic properties but so far it is difficult to see the benefit to our hospitalized patients, but we are using it and the studies will tell. With Plaquenil's potential QT prolongation and liver toxic effects (both particularly problematic in covid 19 patients), I am not longer selectively prescribing this medication as I stated on a previous post.
We are also using Azithromycin, but are intermittently running out of IV.
Do not give these patient's standard sepsis fluid resuscitation. Be very judicious with the fluids as it hastens their respiratory decompensation. Outside the DKA and renal failure dehydration, leave them dry.
Proning vented patients significantly helps oxygenation. Even self proning the ones on nasal cannula helps.
Vent settings- Usual ARDS stuff, low volume, permissive hypercapnia, etc. Except for Peep of 5 will not do. Start at 14 and you may go up to 25 if needed.
Do not use Bipap- it does not work well and is a significant exposure risk with high levels of aerosolized virus to you and your staff. Even after a cough or sneeze this virus can aerosolize up to 3 hours.
The same goes for nebulizer treatments. Use MDI. you can give 8-10 puffs at one time of an albuterol MDI. Use only if wheezing which isn't often with covid 19. If you have to give a nebulizer must be in a negative pressure room; and if you can, instruct the patient on how to start it after you leave the room.
Do not use steroids, it makes this worse. Push out to your urgent cares to stop their usual practice of steroid shots for their URI/bronchitis.
We are currently out of Versed, Fentanyl, and intermittently Propofol. Get the dosing of Precedex and Nimbex back in your heads.
One of my colleagues who is a 31 yo old female who graduated residency last may with no health problems and normal BMI is out with the symptoms and an SaO2 of 92%. She will be the first of many.
I PPE best I have. I do wear a MaxAir PAPR the entire shift. I do not take it off to eat or drink during the shift. I undress in the garage and go straight to the shower. My wife and kids fled to her parents outside Hattiesburg. The stress and exposure at work coupled with the isolation at home is trying. But everyone is going through something right now. Everyone is scared; patients and employees. But we are the leaders of that emergency room. Be nice to your nurses and staff. Show by example how to tackle this crisis head on. Good luck to us all."[\Quote]
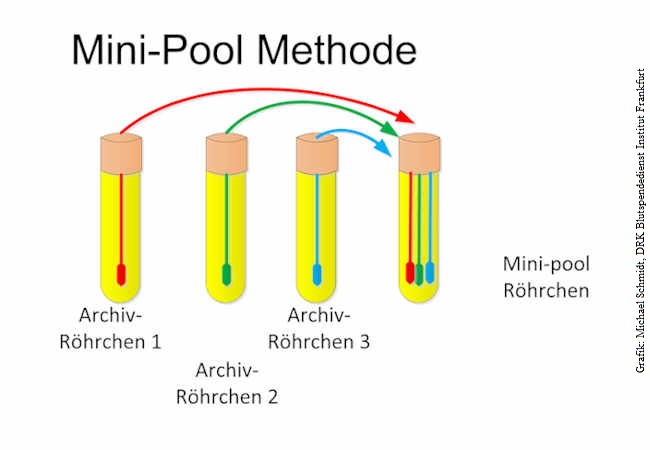
Pool testing of SARS-CoV-02 samples increases worldwide test capacities many times over
Researchers at the German Red Cross Blood Donor Service in Frankfurt headed by Professor Erhard Seifried, and the Institute for Medical Virology at the University Hospital Frankfurt at Goethe University headed by Professor Sandra Ciesek succeeded in developing a procedure that makes it possible to immediately and dramatically increase worldwide testing capacities for detecting SARS-CoV-2.
"This makes it possible for the implementation of expanded testing in larger population groups as demanded by all scientists and also politicians to be carried out sooner than previously thought, even in view of limited test kit resources," says Seifried. The background of this news are laboratory investigations in which swab samples from mucous membranes of the throat or nose are combined using specified procedures in a buffer solution, and subsequently tested using what is known as the PCR procedure (polymerase chain reaction procedure, direct genome detection of SARS CoV-2). In the case of a negative result, all included samples have a reliable negative result. The pool testing has no influence on the detection limit. In the case of a positive mini-pool result, individual testing is carried out in previously reserved samples. The positive sample can then be identified within 4 hours.
"On the basis of these laboratory results, in particular large cohorts and testing on asymptomatic individuals can be carried out, allowing a massive savings of test kits in particular," says Ciesek. The research group is currently analysing options for further enlarging the pools. "The results give cause for optimism that when globally established, the procedure will quickly enable better information about the number of people actually infected," explains Professor Schmidt from the Blood Donor Service.
To continue efficiently implementing the strategy of early detection and isolation, an extension of screening tests is essential, especially for system-relevant professions such as doctors, nurses, police, firefighters, nursing homes, administration and the food industry.
Goethe University President Professor Birgitta Wolff describes the new analysis method as a "milestone". "The more people who can be reliably tested for SARS-CoV-2, the faster the pandemic can be curbed."
 aktuelles.uni-frankfurt.de
aktuelles.uni-frankfurt.de
Not sure if everyone here has seen this already, a high school friend of mine is a nurse and posted this from a doctor she works with on her FB:
Day 10 multi organ failure scared the fuck outta me. That and bilat pneumonia showing up in asymptomatic patient after an X-ray for his shoulder.
 www.webmd.com
www.webmd.com
Someone with EVALI may have breathing and digestive problems, along with other symptoms, including:
Some people say their symptoms formed over a few days, while others say it took several weeks. Those affected seem to have serious lung damage. They may even need intensive care and support with a ventilator, a machine that helps you breathe.
The average age of people with EVALI is 24, and almost 4 out of 5 are younger than 35. Rachel Boykan, MD, a clinical associate professor of pediatrics at the Renaissance School of Medicine at Stony Brook University, says that might be because vaping products are most popular with younger people.
Yeah, but you can't just assume that and pretend people will be immune. We still don't know what kind of immunity we're dealing with, you can't just let people out based on no actual evidence.That's how allll viruses work Fauci said something similar in a..YouTube interview with that ughhhh Defranco guy
You are basing that off one tweet? Aren't there a few studies floating around showing that while it's not a magic bullet it helps?
That above quote from the ER Dr had a stat that something around 86% of people on ventilators die?? The last number I saw was something around 50% and THAT scared the hell out of me. 86% is insane. Is there any other data on this? Maybe at this rate it's better not knowing...
I remember back when I developed fever and back pain three weeks ago that I read the average progress of the disease on the WHO site. It went something like thisNot sure if everyone here has seen this already, a high school friend of mine is a nurse and posted this from a doctor she works with on her FB:
Day 10 multi organ failure scared the fuck outta me. That and bilat pneumonia showing up in asymptomatic patient after an X-ray for his shoulder.
I remember back when I developed fever and back pain three weeks ago that I read the average progress of the disease on the WHO site. It went something like this
Day 1 lower back pain and mild fever. - Yep.
Day 3 slightly higher fever, fatigue and dry cough - Yeah that's where I'm at now.
Day 6 mild symptoms
Day 8 death - WTF
But this is shocking to me, damn:
Makes you wonder if the rapid dash for more ventilators even is very meaningful.
Edit: makes sense that this is the number if you put everyone on ventilator yeah, theres a reason how here in the Netherlands most people 80 and up are strongly discouraged to go to the ICU (or even denied).
I remember back when I developed fever and back pain three weeks ago that I read the average progress of the disease on the WHO site. It went something like this
Day 1 lower back pain and mild fever. - Yep.
Day 3 slightly higher fever, fatigue and dry cough - Yeah that's where I'm at now.
Day 6 mild symptoms
Day 8 death - WTF
But this is shocking to me, damn:
Makes you wonder if the rapid dash for more ventilators even is very meaningful.
Edit: makes sense that this is the number if you put everyone on ventilator yeah, theres a reason how here in the Netherlands most people 80 and up are strongly discouraged to go to the ICU (or even denied).
This is how countries will bridge the gap until a viable vaccine is produced.
That 86% is extracted from a Chinese paper.I remember back when I developed fever and back pain three weeks ago that I read the average progress of the disease on the WHO site. It went something like this
Day 1 lower back pain and mild fever. - Yep.
Day 3 slightly higher fever, fatigue and dry cough - Yeah that's where I'm at now.
Day 6 mild symptoms
Day 8 death - WTF
But this is shocking to me, damn:
Makes you wonder if the rapid dash for more ventilators even is very meaningful.
Edit: makes sense that this is the number if you put everyone on ventilator yeah, theres a reason how here in the Netherlands most people 80 and up are strongly discouraged to go to the ICU (or even denied).
I'm giving the benefit of the doubt that you don't mean the bolded quote in the way it appears.
I say this because under no circumstances is saving 14% not worth it.
If you didn't have more ventilators because it wasn't very meaningful it's absolutely possible that those 14% may have died too.

That 86% is extracted from a Chine paper.
From this article, it seems that for other countries it may be different:
Mortality rate of COVID-19 patients on ventilators - Physician's Weekly
Written by Physician's Weekly Blogger, Skeptical Scalpel Although at the time I wrote this over 33,000 people had died from COVID 19 infections worldwide, the numbers of patients dying in intensive care units and on mechanical ventilation is unknown. We have some early published data on...www.physiciansweekly.com
Right, statistically if you are intubated above the age of 80, your likelihood of living isn't great and I'd imagine the 14% of people this doc is talking about are going to be younger patients. My wife intubates daily and even normal procedures, intubation for someone that old is super risky and even if they survive the procedure, the likelihood of meaningful recovery isn't the best which is why it's avoided as much as possible.
Speaking of ethnics and such this is a good article that came up that's going around the medical field.
U.S. Civil Rights Office Rejects Rationing Medical Care Based on Disability, Age (Published 2020)
Medical providers must not engage in “ruthless utilitarianism” in deciding who gets lifesaving treatment for the coronavirus, a federal civil rights officer warned.www.nytimes.com
It most likely is inflated but apparently most people who go on a ventilator end up dying. The longer you need it the higher the risk of death becomes.
 apple.news
apple.news
Not sure if everyone here has seen this already, a high school friend of mine is a nurse and posted this from a doctor she works with on her FB:
Day 10 multi organ failure scared the fuck outta me. That and bilat pneumonia showing up in asymptomatic patient after an X-ray for his shoulder.
A little rant.....So I work Off Duty Employment for a grocery store in the Indianapolis area. The past several locations I've worked, I've watched store employees horde key items such as toilet paper, lysol, disinfectant wipes to where there is no more product left or very few left on the shelf prior to the store opening. During operating hours, I've watched these same employees tell customers they are only allowed 1 item of these key items that are in such high demand and take the extra items out of the elderly persons cart. Now, I completely understand the 1 item rule and I believe the employees should adhere to their own rules as well. This is why most grocery stores are out of these key items because employees take them off the shelf before opening and purchase more than the 1 item allowed per store rules. For example; I watched 1 employee take 4 cans of Lysol and 3 things of toilet paper of 6 off the shelf and purchased it. This same employee took an extra toilet paper package out of an elderly persons cart because of the 1 item rule. This just really upsets me. Maybe I'm overreacting, but I don't think that's fair especially when product is low.
I hope he makes a speedy recovery! Please keep us updated.
Not sure if everyone here has seen this already, a high school friend of mine is a nurse and posted this from a doctor she works with on her FB:
Day 10 multi organ failure scared the fuck outta me. That and bilat pneumonia showing up in asymptomatic patient after an X-ray for his shoulder.
A nursing home in Canada with an outbreak pretty much tell the family: Even if the senior survive the tube their quality of life will greatly diminish. So think twice before sending them to hospital.

When I was a kid I always saw USA like an utopian country where everything was possible. As I grew up all that utopian image I had just vanished as more as I understood the system (specially the health care system) . As of right know I'm really baffled how could anyone like trump be the president of such an immense country. How is that even possible? How can the guy still be president after all this horrible management of this pandemic.
apple.news
A spokesman for the Agriculture, Fisheries and Conservation Department (AFCD) said today (March 31) that a pet cat sent to the AFCD has tested positive for the COVID-19 virus. This is the third animal to test positive in Hong Kong, following two earlier cases in which two dogs tested weak positive or positive during repeated tests for the virus.
The current case involves a Domestic short-haired cat that lived in a residence at Aberdeen. When the owner was confirmed with COVID-19, the cat was sent for quarantine at the animal keeping facility at the Hong Kong Port of the Hong Kong-Zhuhai-Macao Bridge yesterday (March 30). The Department has collected samples from the cat for tests, and the oral cavity, nasal and rectal samples were tested positive with COVID-19 virus. The cat has not shown any signs of disease.
Shite. Dogs and Cats now? If legit, does that mean it can extend to rats or birds?Hong Kong - Pet cat tests positive for COVID-19 virus
https://www.info.gov.hk/gia/general/202003/31/P2020033100717.htm
Oh, that's a pretty big jump....Sky News Breaking on Twitter
“NHS England says the number of people in England who have died after testing positive for COVID-19 has risen by 367 to a total of 1,651”twitter.com
367 new deaths in England over past 24 hours (including other countries that make up the UK is likely a higher total)
Firing doctors on a pandemic crisis sounds like a very very bad strategic move.*sigh*
Hospitals Tell Doctors They’ll Be Fired If They Speak Out About Lack of Gear — Bloomberg
Hospitals are threatening to fire health-care workers who publicize their working conditions during the coronavirus pandemic -- and have in some cases followed through.
Lombardia (Italy) update:
+1047 new positive cases (total 43208)
+381 new deaths (total 7199)
It's been mostly answered by now, but I would hazard a guess the statistics are such that at 86% mortality it's even more grim for elderly patients. As said in my country most people die outside of the ICU because in consultation with their physician they weren't brought into the ICU. I was pretty vocally against that, but with these numbers it seems to make sense, given that a) theres only so much doctors capacity (this is a harder limit than the ventilators) b) dying on the IC is horrible, protracted, and you die without your loved ones being allowed near you.I'm giving the benefit of the doubt that you don't mean the bolded quote in the way it appears.
I say this because under no circumstances is saving 14% not worth it.
If you didn't have more ventilators because it wasn't very meaningful it's absolutely possible that those 14% may have died too.
Not sure if everyone here has seen this already, a high school friend of mine is a nurse and posted this from a doctor she works with on her FB:
Day 10 multi organ failure scared the fuck outta me. That and bilat pneumonia showing up in asymptomatic patient after an X-ray for his shoulder.